Society
Society

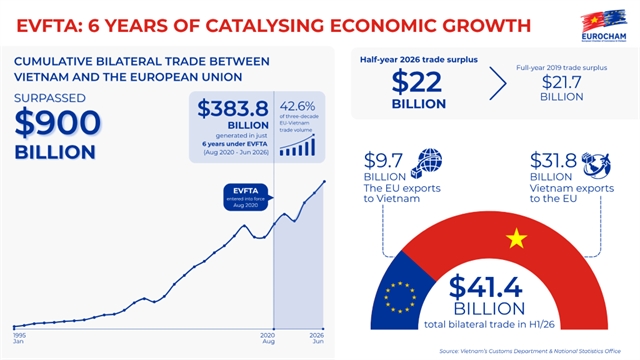
EVFTA reshapes Việt Nam-EU trade six years after launch
1.
.jpg) |
| UNAIDS Regional Director for Asia and the Pacific Taoufik Bakkali talks to Việt Nam News. — UNAIDS/VNS Photo |
On the occasion of the World AIDS Day (December 1), Việt Nam News reporter Trọng Kiên talks to the UNAIDS Regional Director for Asia and the Pacific, Taoufik Bakkali, on the HIV/AIDS situation in Việt Nam and across the region, and paths towards sustainability.
What is your assessment of HIV/AIDS in the Asia-Pacific region and in Việt Nam in particular, before and after COVID-19?
Asia-Pacific has about five million people living with HIV. The characteristic that distinguishes the Asia-Pacific is that it has a concentrated epidemic, mostly affecting “key populations” and their partners. We are talking about people who use and inject drugs, female sex workers and their clients, men who have sex with men (MSM), transgender women, and their sexual partners. Some 96 per cent of all new HIV infections in Asia-Pacific are within these key populations.
There has been some relative success in the region. We are seeing a 26–30 per cent decline in new HIV infections overall. But these average numbers don’t show the major differences in this region. We have countries like Việt Nam, Cambodia and Thailand that have achieved a very strong decline in new infections. But we also have countries with very worrying trends, like the Philippines which has had a 300 per cent increase in infections since 2010 and Pakistan also with a very high rate of increase. I mention these because they have quite large epidemics. There are also countries in the region with relatively small epidemics, like Papua New Guinea, where the trends are increasing. Also, we have countries like Malaysia, where there had been success in the past but now the epidemic is picking up once more and it’s a different epidemic than in the past.
It's good to talk about regional numbers and regional trends, but we must also look closely at the many differences between countries and even within countries, that need to be properly analysed and addressed.
COVID-19 caused disruptions to all health systems. Everything went into the COVID response: vaccination programmes stopped, TB programmes stopped, STI programmes stopped, HIV programmes stopped in almost every country because everything was for a certain period diverted to the COVID response. And this, naturally, had an impact on the HIV response itself and the trend of the epidemic. We have seen a lot of losses. For example, we were seeing about a 10 per cent gain on ARV treatment enrolment every year regionally, then COVID came and the growth in enrolment dropped to 5 per cent.
So COVID did have an impact and slowed down the progress. This comes in a context where we had a strategy with the 95-95-95 targets for 2025 [in which 95 per cent of people living with HIV are tested and know their status; 95 per cent of people who know they are HIV-positive are on treatment; and 95 per cent of people on treatment achieve viral suppression, meaning they cannot transfer the virus sexually]. Then we had three years that not only slowed down progress, but in some countries the AIDS response went backwards due to COVID-19.
But we also have seen a number of new innovations, new solutions being put in place, and decisions being taken very quickly. In many cases, we have seen community organisations engaging to ensure people have access to the services that they need. Some bring medicines to people who are locked down in their homes, and they were connecting them to treatment facilities even during lockdown. And there were many other models of service delivery including using online virtual spaces to provide support for accessing prevention and treatment services. Those innovations turned out to be very, very effective and they sent us in the direction that we would call the ‘new normal’ now in the HIV response.
Speaking of COVID-19, do we need to worry about the variants of HIV/AIDS, or what could we do when the next pandemic hits to shield the HIV response from the worst impacts?
We have learned from pandemics, including AIDS and COVID-19. If you look at the Global AIDS Strategy 2021–2026, it has very strong components on pandemic preparedness regardless of what virus or variant that is, including building up resilient systems for readiness and response, whether it is variants of COVID or something else like monkey pox or something new that will emerge. What are the systems in place to ensure that we don't lose the gains in other areas? We have to consider what are the systems now? Taking learnings from that experience, what needs to be in place without waiting for a pandemic to be declared? So that is the investment that needs to be happening now. That's why we are focusing on community leadership, innovation, resilient systems, and systems for health beyond health systems. All of these help in the response to HIV and COVID-19, and in preparing for any future pandemics.
We cannot wait for a pandemic to come and then say, okay, let's build something new. We need to have it in place so that we are resilient and well prepared and able to respond immediately.
You mentioned increasing prevalence of HIV among the younger generation especially in high-risk groups. Can this issue threaten Việt Nam’s goal of ending AIDS by 2030?
One of my main objectives in this visit is to highlight the success story here. What has worked in Việt Nam is dedicated, evidence-informed strategies that target the right populations in a very effective way. The problem that we have learned in a hard way, is that the epidemics do not remain the same, particularly HIV; the dynamics of infection keep changing.
Recently, until 2011-12, the Philippines did not have many HIV infections. Now it has one of the highest increases in the world, mostly affecting men who have sex with men. Recently, Malaysia was a good success story that we were celebrating, just like Việt Nam’s, because they were responding to the epidemic among people who inject drugs. But now Malaysia is one of the countries with an increasing trend compared to the baseline of 2010. So, all the gains that were achieved in the past are offset. Infections are not increasing among people who inject drugs but among MSM.
This brings me to the analogy with Việt Nam. We're going to take the success of the past, which is a successful programme targeting people who inject drugs, with good control of the epidemic leading to about 69 – 70 per cent decline of new infections. This is huge. That's the best in the region right now. But we are also seeing signs that the epidemic is increasing among specific populations, particularly young MSM. A Malaysia-like situation could be avoided if we have immediate action taken and at large scale here.
Việt Nam has recently started to offer PrEP (Pre-exposure prophylaxis) to people at high risk of HIV infection. We know that PrEP is highly effective in preventing new infections, particularly among MSM, sex workers and others. Việt Nam adopted this even before we started getting those indications. But is it being implemented at a large enough scale to avoid a possible reversal of the trend? We don't yet know: it depends on what happens next. So yes, there is still a risk here.
It is very important to look closely at who is most at risk, and who is being left behind. We cannot simply rely on national or regional trends. We must look carefully at the details. This is why the theme of World AIDS Day this year is about inequalities, or “Equalise.” How do we equalise the AIDS response, by improving our understanding of sub-populations who remain vulnerable? Their vulnerability can be due to some risk behaviours, because they don't access services, or because of transmission dynamics. So, we need to look into the details and understand whether the factors are geographic, or whether specific sub population or age groups etc. are especially vulnerable, and then we will understand how new infections are affecting specific parts of the population, why they are increasing, and how we must respond to it. That is how we can control the overall epidemic.
What are your recommendations for Việt Nam in its national strategies against HIV? Especially when Việt Nam is now in the middle-income group, which means international HIV assistance – funding and other resources in particular – will gradually be phased out, and the country will need to work on its financial self-reliance.
After 40 years of the HIV response, we have the tools, the understanding and the community and political support needed to reduce new infections and AIDS-related deaths. But we have still not reached epidemic control. We have made lots of progress, but the future requires different things. First on the programmatic side, we need to focus on sub-populations where most new infections are happening. We know this from modelling, but also from reported cases, that the greatest risk is among young people and especially those in key populations. Now if you want to focus on that, you need to bring innovation to service delivery. It is not enough to introduce virtual connection to services, or even to launch a national PrEP programme, because there is also a need for supportive policies, and to scale up effective programmes to a wide scale. Việt Nam is a large country with a sizable population, and the epidemic is relatively large compared to other small epidemics. So solutions need to be implemented at scale.
Việt Nam has been praised for being the first country in this region to announce the nationwide rollout of PrEP, before Thailand in 2019. But since then, the number of users has only reached 30,000 which is quite small.
When we consider innovative service delivery in the virtual space, it's not enough to have it in a pilot in one province, or one city. We need to go beyond pilots and trials, and provide more access to these innovations.
On the policy side, we need communities and community-based organisations to be engaged in supporting the scale-up of service delivery models. We understand the governance system and the challenges here in Việt Nam and the required transition, particularly with regard to capacity building of civil society and community organisations, to be able to deliver on service delivery. So that's a request for policies that need to be adopted, in addition to allowing for innovative models of service delivery to be implemented.
When we talk about community engagement, we must consider financing the AIDS response, as you asked. First, we need to ensure the transition of financing sources, and scaling up, to increase financing from domestic resources so that we can meet the needs of that scalar. But at the same time, there is a need to find or develop innovative sources of funding. So, it cannot only depend on central government funding. We have seen in other countries that there are various ways to do it. Many countries are looking at their health insurance and how they fund universal health coverage, which is a Sustainable Development Goal. There are various mechanisms to mobilise additional resources for service delivery, for ways for those services to be funded. And then you add to this the other element, which is related to the community role. Now communities, if they are going to provide that service, they need to access funding. That's why we are looking at the financial sustainability of community organisations, which is one specific element of the sustainability of the overall AIDS response.
All these are elements that need to be considered, as the AIDS response evolves from where we are right now.
During the transition of Việt Nam into financial self-reliance, should people who are now on PrEP be worried about a potential disruption when the pills might no longer be free? Will ‘having to pay’ discourage usage?
That's where the financing discussion and sustainability discussion is very pertinent. There are various models and we need to find what's the solution that works best here, because when we talk about vulnerable populations, for example, young MSM aged 15-24 usually do not have disposable income for health services, yet you need them to be protected. To stop the pandemic, the people at the greatest risk of infection need reliable and affordable access to prevention measures, so we need to find a sustainable financing solution. And there are various ways, different mechanisms.
Thailand, for example, included this under its approach to universal health coverage, with a national insurance system that helps finance service delivery, with contributions from government as well.
I agree that it is not acceptable to create dependency for HIV prevention based on self-paid services or user fees. Although in some situations, in some models of public health service delivery, there is some tolerance towards user fees for those who can afford it. But we cannot assume that everybody can afford it. So naturally, prevention services including PrEP need to be available through a mechanism of financing that would not create or increase inequalities in access. A situation where access is only for the rich, the privileged and those who have money is not acceptable — that is not the principle of the AIDS response. If we continue like that, we will never end the AIDS epidemic.
Does this mean that private insurance can cover HIV prevention and treatment?
There are different ways. Look at the Philippines, which has a very decentralised governance system, here, local governments are mandated to liaise with insurance companies. In case of China, those decisions are taken at the central government level. In India, all HIV prevention services paid for centrally through a contracting mechanism. The HIV response, particularly access to prevention, is essentially funded through community organisations, which means no need for an insurance scheme in that system, because it's already provided by governments and delivered by communities. So, these solutions need to be adapted, and ideally there should be a mix of options that will ensure everybody is covered.
 |
| A communication officer observes harm reduction intervention services for men who have sex with men in the northern province of Hải Dương. — VNA/VNS Photo Dương Ngọc |
Can we talk more about the social contracting, where community-led HIV/AIDS services and delivery are paid for by the State? Is that a practical approach for Việt Nam?
This requires a bit of adaptation. It's not a model that can be imported and easily implemented in every country because each country has its own governance system and financing schemes.
Social contracting is being piloted in a number of countries. The services and the mechanism for delivering them are different. Here in Việt Nam, which is very interesting since you have a more advanced model, it is called social enterprises. It requires very strong organisations in terms of capacity and financial management and the term ‘enterprise’ suggests that organisations might make money from their services. That is different from social contracting, but it is a system already in place that can be built on. One challenge is that social enterprises must have technical, financial and programmatic capacity, which means that you cannot have many smaller enterprises, but instead you will have very few larger enterprises, which creates limitations.
In China, social contracting involves even non-registered, local community-based organisations or civil society, which can access funding from the central government and provide services for HIV services for target populations. The same happens in India, though with significant differences. You have a specific contract for a specific amount for a specific number of people. If you can deliver that service, you get the contract, and you report how many people were reached, how many people received condoms, how many received PrEP etc. In the Philippines, the model is rather about reimbursements, you have organisations that are recognised, that deliver services and then report and claim reimbursement from the State.
So there are different models around the same principle of accessing funds through the government in various ways, to contract community organisations to deliver a specific service.
What would work best for Việt Nam is, I think, something that collectively Việt Nam needs to work out together with its partners. I know that social contracting is being piloted in seven provinces and that UNAIDS is supporting one province, and there are lots of learnings from that in terms of costs, service delivery, reporting, and target setting. We need to see how this pilot will work, but it's good that it's already started. I hope that the pilot does not go for very long, so we can determine what works and immediately scale it up to all provinces.
In Việt Nam, the model is half-and-half, for example, upon the contract there will be an advancement of about 30 per cent of the funding, and then the organisations will deliver the services, report on the results, and receive the balance of funds. It’s basically performance-based. There is no hard and fast rule about how this should be structured.
Is UNAIDS supporting social enterprises and other community-based organisations in Việt Nam, and how?
Yes. This is a crucial element and part of our overall approach. It reflects the Global AIDS Strategy goal of financial sustainability and equitable financing. The term equitable means not only bringing money, but also not leaving anyone behind. In this context, UNAIDS works with all countries depending on their needs, not only in supporting the piloting of social contracting, but also generating the evidence, designing the package to address the gaps and reflecting what works, using allocative efficiency, and analysing the models of service delivery. So that we can advocate for the right mix of investment approaches that will give us the maximum results.
We know that COVID not only had an impact on the response to HIV and other health conditions; it also had impact on economies. So, while we are arguing for sustainability and domestic financing, we understand that not all countries can immediately generate the domestic resources necessary to replace international sources. So, we need to see how to make gains within the available resources, and this means having better allocation, to get the maximum results from that money. When we look in detail, we might find that some forms of service delivery are very expensive for what they achieve, or they might have components that we can change to achieve better results with the resources. Community-led responses can be cheaper, except for the initial investment. Virtual space and outreach can be cheaper, but you might need to invest more in commodities and less in service providers.
So, there is a balancing needed to save on the service providers who, instead of having them confined to a clinic, can be made available through the computer, or by delivering condoms, self-test kits and medicines. You might even save some money.
UNAIDS and our partners, including PEPFAR (the United States President's Emergency Plan For AIDS Relief) and the Global Fund, are very interested in providing support to this analysis and understanding how to make the most of the available resources.
With COVID’s impacts on the economy, can we expect international partners to be more willing to continue their assistance to less developed countries, including Việt Nam, in HIV response for some more years, to cover up for the lost time caused by COVID?
We hope so. There is a lot of advocacy being done, but nothing is guaranteed. And we know that there are various pressures on all countries, including the big economies, so I think we need to be prepared for all scenarios.
We do see a declining trend of international contributions to the HIV response globally, not just in Việt Nam, so we need to start preparing for the transition to domestic resources.
At best, we can advocate for the reduction in international support to slow down, but nothing is guaranteed because of the complex politics and economic factors that underlie international donations. We cannot just wait; we have to prepare for alternative options that are not only domestic central-level funding. So that's why we're talking about UHC, insurance, and various mechanisms to mobilise resources and improve efficiencies. It is not only the concern of central government: it could be local governments and a combination of solutions and stakeholders that would help transition the HIV response towards sustainability.
What can we do to ensure the sustainability of community-based organisations and community-led responses. What might be practices from other countries that can be replicated, and challenges that may be facing them now?
I'd like to see the sustainability of community-based organisations embedded in the broader discussion of financial sustainability of the HIV response. When you look at the financial stability of these organisations, and the services they deliver, the people involved and the benefits it brings to the AIDS response, it offers a different dimension than just how much money is available. It opens the opportunity to consider transitioning some models of service delivery towards community leadership, for example.
And when we talk about community leadership, it raises the issue of different roles and functions and how communities are involved. Social contracting — where communities are paid to deliver services — empowers community organisations to access funding to deliver services, whether for service delivery for prevention or treatment or for testing. But these contracts can create financial dependence that limits their role in leadership and advocacy. To be effective advocates for their communities, and to have a role in monitoring the effectiveness of the AIDS response, they need to feel relatively more independent and empowered, with their own resources. That leadership role requires more than access to funding to deliver services.
The sustainability of those additional resources is also a challenging issue right now. Should community organisations rely on international sources, so they maintain independence locally? Or do should they move towards the model I mentioned, of social enterprises that generate income from services? Can a revenue-generating enterprise be an effective advocate for the people who become their clients? Can they be activist for people being left behind? Can an organisation that provides services also evaluate their own delivery and advocate for improved quality?
There are still discussions needed about what works, and UNAIDS will help share the results of pilots and efforts across the region. The whole concept of community-led response is relatively new, and we expect it to be better defined very soon.
For now, we're still working on the elements for reaching the targets for service delivery, with at least 80 per cent of prevention targets, 30 per cent of testing and treatment, and 60 per centof advocacy and programmatic investment in enabling environments, which is to change the policies and laws and acting on stigma discrimination. Some of these cannot be quantified or solved with a single formula, particularly if we are talking about funding coming from domestic resources.
There is a bit of more work that needs to be done in this area, and we are working with regional organisations and networks, and we hope that they will strengthen the capacities and help us establish the solution at the country level.
Hopefully, that's something that will be worked out during the course of next year or in the immediate term because if we want to foster community leadership, we cannot avoid talking about financial independence. — VNS
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society
 Society
Society