Life & Style
Life & Style

Sacombank tells shareholders most business targets achieved in 2023
1.
|
By Dr Olivia Wyatt*
The World Health Organization (WHO) recommends that women breastfeed exclusively for their baby’s first six months of life, without the need for additional solid food or fluids – including water. UNICEF data suggests that 24 per cent of babies in Việt Nam are in fact breastfed up to the age of six months, higher than the overall global rate.
Breastfeeding reduces the risk of many diseases that are a threat to infants, including Sudden Infant Death Syndrome (by 36 per cent); middle ear infection, allergic rhinitis, and childhood leukemia (by about 18 per cent). There are also studies that show children who are breastfed tend to have a higher IQ, and are less likely to be obese or overweight in adolescence and adulthood.
The benefits to the mother of breastfeeding include a reduced risk of pre- and post-menopausal breast cancer (because of a reduced exposure to estrogen) and a reduced risk of ovarian cancer. These benefits increase with longer periods of breastfeeding.
Despite these benefits, it’s unfortunate that some mothers do experience significant challenges in breastfeeding their babies. About 30 per cent of women have at least one breastfeeding problem during the first two weeks after delivery, most commonly the baby rejecting the breast, as well as painful breasts/nipples.
After the first few weeks, the most common reason for stopping breastfeeding is reported as insufficient milk – which can include the perception of insufficient milk. Appropriate management and support for these problems is key to achieving ongoing breastfeeding.
Not all mothers who worry about low milk supply have an actual issue. Milk production is a feedback mechanism – the more you feed, the more milk is produced, and the less you feed, the less milk is produced – so if the mother starts supplementing breast milk with bottle feeding, this may lead to an actual decrease in her milk production.
Sometimes there really is an issue with milk transfer, in that the milk isn't being effectively withdrawn from the breast by the baby. The most common cause of this isn't an illness – it's more to do with positioning and attachment of the baby at the breast. If the mother is not positioned correctly while breastfeeding or the baby is not attached to the breast well, it will become more painful and lead to ineffective milk transfer.
Rarely, in perhaps 2–5 per cent of cases, there is an underlying medical problem. Issues such as retained placenta, hyperthyroidism and heavy bleeding during delivery can affect the pituitary gland, which affects milk supply. A third of women who have polycystic ovarian syndrome will have problems with their milk supply – breast surgery can also be responsible for this situation, as can the effect of hormonal contraception.
Pain in breastfeeding can have a significant impact on the relationship and whether the mother chooses to continue breastfeeding her child. Cracked or sore nipples are common and are usually due to positioning and attachment issues. Usually with practice and patience, the issue resolves itself and the woman can carry on without needing to see a doctor. Breastfeeding isn’t supposed to be painful, and if the problem continues for a long period, it is advised for the mother to seek help from a medical or health professional.
Trained healthcare professionals can support mothers and educate them about the best positions for the strongest attachments. Usually, if the nipple is brushed against a baby's top lip and nose, it will fully open its mouth. This is called rooting, and every suckling animal has the same instinctive response. It will latch on naturally when the nipple touches the top of the mouth, which draws in quite a large part of the breast rather than just the nipple. If the mother and baby are properly guided, the baby will get used to the correct rooting response, and the more frequently it will occur.
A lactation consultant – or a midwife, or a nurse – can help to educate new mothers on how breastfeeding works, what to expect, what's normal, and what's not often talked about, especially in the early stages. — Family Medical Practice
*Dr Olivia Wyatt was born in South Africa and raised in Botswana, where she worked with HIV patients with Harvard Medical School and the Clinton Foundation. Now a mother of two, Dr Olivia regularly convenes FMP’s Saigon International Mother and Baby Association, a group supporting new and expecting mothers with parenting guidance and information, where she leads discussions on topics such as feeding, sleeping, development milestones, colds & coughs, and vaccinations over coffee, tea, and cakes.
Family Medical Practice was the first foreign-owned primary healthcare provider in Việt Nam, and has consistently remained at the forefront of international-standard medicine since 1995. It offers extensive healthcare and emergency medical services nationwide to Vietnamese, expatriate and corporate customers.
For more advice on any medical topics, visit Family Medical Practice Hanoi at: 298 I Kim Mã, Ba Đình. Tel: (024) 3843 0748. E: hanoi@vietnammedicalpractice.com.
FMP’s downtown Hồ Chí Minh location is: Diamond Plaza, 34 Lê Duẩn, District 1; 95 Thảo Điền, District 2. Tel: (028) 38227848. E: hcmc@vietnammedicalpractice.com
FMP ĐàNẵng is located at 96-98 Nguyễn Văn Linh, Hải Châu District, Đà Nẵng. Tel: (0236) 3582 699. E: danang@vietnammedicalpractice.com
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
The Việt Nam Fatherland Front Central Committee in HCM City and HCM City Television, in co-cperation with their partners, will broadcast a special music programme on Vietnamese seas and islands tomorrow (August 29) to mark the 74th anniversary of National Day (September 2).
 Life & Style
Life & Style
Historian and teacher Nguyễn Thừa Hỷ won the 'Bùi Xuân Phái – For The Love of Hà Nội' prize on Tuesday at Vietnam News Agency’s headquarters.
 Life & Style
Life & Style
Reporter Quỳnh Yên, from Sài Gòn Giải Phóng (Liberated Sài Gòn) newspaper talks to her about her work.
 Life & Style
Life & Style
 Life & Style
Life & Style
Designer Phương My exhibited her first bridal collection “Espoir” (Hope) at HCM City’s Park Hyatt Saigon last Friday.
 Life & Style
Life & Style
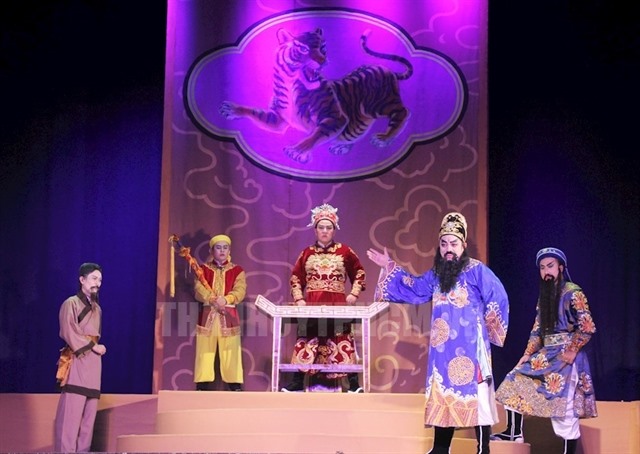
The HCM City Hát Bội Theatre will launch a new programme offering hát bội or tuồng (classical drama) performances for foreign visitors as part of the theatre’s efforts to introduce Vietnamese theatre to the world.
 Life & Style
Life & Style
The annual symphony concert "Điều Còn Mãi" (What Remains Forever) hosted by online newspaper Vietnamnet will be held for the 10th straight year on September 2 at the Hà Nội Opera House.
 Life & Style
Life & Style
 Life & Style
Life & Style