 Life & Style
Life & Style


Impressive growth poses macroeconomic balancing challenge: experts
1.
" />Do you shiver in the cold? If you do then you handle it better than some people. Without our protective mechanisms, the body’s core temperature can quickly drop and there is a risk of frostbite. At the same time, a body that is cooled down copes better without oxygen, something which researchers can utilise to save lives.
 |
| Dr. Mattias Larsson — Photo courtesy of Family Medical Practice Hanoi |
By Dr. Mattias Larsson*
Do you shiver in the cold? If you do then you handle it better than some people. Without our protective mechanisms, the body’s core temperature can quickly drop and there is a risk of frostbite. At the same time, a body that is cooled down copes better without oxygen, something which researchers can utilise to save lives.
We are now entering the cold season. Researchers have started to use the fact that when the temperature of our bodies goes slightly down we need less oxygen to treat newborn babies that suffer from asphyxia or lack of oxygen at the moment of birth, helping the plasticity/restoring mechanisms of these children’s brains.
Cold can damage us in two ways; either through localised frostbite on a body part, or through hypothermia, where the core temperature of the body sinks.
The body’s main defence against cooling is shivering, and how effectively we shiver is also individual. This causes the muscles to release energy, providing warmth and keeping the body temperature up. But some people do not shiver at all and are unprotected against the cold. The lower the body temperature, the lower the metabolism. This means the organs use less oxygen, for example.
It is this mechanism that is now being consciously used in several ways in healthcare. In cases where patients have oxygen deprivation of the brain, called asphyxia, due to example decreased blood flow – which is one of the most common complications during delivery – cooling has been shown to be an effective way of saving the brain.
By beginning cold treatment early within the first six hours, we think there is potential to save the nerve cells that die as a result of oxygen deficiency. The brain is stressed as a result of oxygen deficiency and a cascade of biochemical processes begins. For example, the nerve cells begin unrestrainedly producing the signalling substance glutamate, something which ultimately results in an excess of calcium – leading to the death of the nerve cell. Slowing down the brain’s metabolism by early cooling may be one way to reduce this excessive production of glutamate.
For neonatal care the cooling treatment lasts for 72 hours. Sweden was one of the first countries in the world to introduce cooling treatment for children with acute oxygen deficiency. About one quarter can be kept alive or saved from severe brain injury by cooling. Despite this, not all children receive the treatment they need since it must be initiated within six hours of birth. Because the majority of hospitals cannot offer proper cooling, the frail, newborn babies must be immediately transferred; a decision requiring quick actions on the part of a skilled paediatrician. During the transfer, the child is often placed in a normal transport incubator.
There is a need for simpler and safer transfers of children who need cooling treatment. Linus Olson, PhD, and a civil engineer and researcher at the Karolinska Institutet currently working in Vietnam, is involved in a research study testing a cooling mattress on newborn children with acute oxygen deficiency. The mattress works without either electricity or water, which means it can be used in all ambulances and hospitals. It is made of a plastic shell filled with something called phase-change material, which can transform from a solid to a liquid, using the child’s body heat as a source of energy in the process. After about an hour on the cooling mattress, the child reaches a temperature of about 33.5 degrees. A big plus is that the mattress then maintains this temperature in a stable way. It is also a lot cheaper that the equipment currently used for cooling treatment. In addition to the opportunity to improve transfers, we see the potential for improved neonatal care all over the world. Cooling treatment is currently introduced in hospitals in Vietnam. In this study, the mattress will be used to deliver cooling treatment at several hospitals and during transport. The goal is to save lives and reduce brain injuries among children with acute oxygen deficiency. So far the study confirms that the mattress is effective in these contexts, and there are plans to introduce it more permanently in neonatal care in Vietnam. In the long-term, other countries with less developed neonatal care will be of interest. The cooling mattress is also being tested in a study in Sweden. In the first stage, newborns with oxygen deficiency will be randomly selected to be transferred by air, either in a normal transport incubator or on the cooling mattress.
Cooling to protect the brain may help more patient groups than it is currently being used for, such as stroke patients or cardiac arrest patients. However, these people are often conscious, and then need to be anaesthetised. Cooling treatment may be refined further in the long-term, with better data concerning what body temperature is actually optimal and how long the cooling should last. — Family Medical Practice
*Dr. Mattias Larsson first came to Vietnam in 1997 conducting research on child infections and antibiotic use and resistance. In 2003 he defended his PhD and graduated from his medical training. Since then he has spent about half of his time in Sweden working as a physician in pediatrics and infectious diseases, and the other half in Việt Nam and other developing countries working on medical training and research. Dr. Mattias speaks English, Swedish, German and Vietnamese as well as some Spanish. He will complement the team at Family Medical Practice, and intends to participate in the development of diagnostics care and treatment towards best international evidence-based standards.
For more advice on any medical topics, visit Family Medical Practice Hanoi at: 298 I Kim Mã, Ba Đình. Tel: (024) 3843 0748. E: hanoi@vietnammedicalpractice.com.
FMP’s downtown Hồ Chí Minh location is: Diamond Plaza, 34 Lê Duẩn, District 1; 95 Thảo Điền Street, District 2. Tel: (028) 38227848. E: hcmc@vietnammedicalpractice.com
FMP Đà Nẵng is located at 96-98 Nguyễn Văn Linh Street, Hải Châu District, Đà Nẵng. Tel: (0236) 3582 699. E: danang@vietnammedicalpractice.com
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
 Life & Style
Life & Style
Designer Đỗ Trịnh Hoài Nam will present a collection of áo dài (traditional long robe) embracing brocade patterns during a festival dedicated to brocade held in the Central Highlands province of Đắk Nông on January 5-7.
 Life & Style
Life & Style
Football fans throughout the country have been counting down the minutes until the kick-of of the AFF Cup final's second leg, with Việt Nam taking on Malaysia at Mỹ Đình Stadium in Hà Nội.
Millions of Vietnamese have faith their heroes will bring the cup home.
 Life & Style
Life & Style
A traditional fire dance of the Red Dao ethnic minority group in the northern province of Điện Biên has been restored after 20 years thanks to efforts made by the provincial museum, local authorities, elders and researchers.
 Life & Style
Life & Style
The HCM City Department of Culture and Sports will launch a month-long programme featuring traditional Vietnamese performing arts to celebrate 100 years of cải lương (reformed opera).
 Life & Style
Life & Style
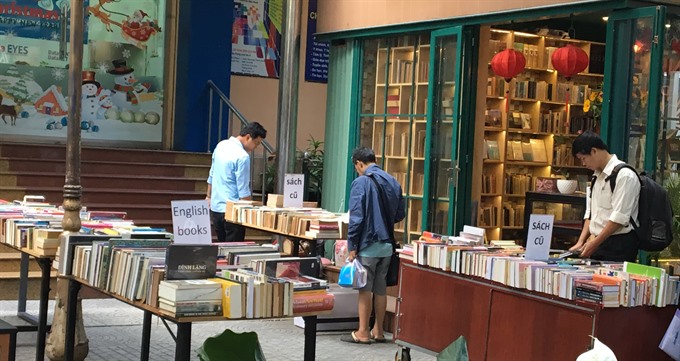
The HCM City-based Trẻ (Youth) Publishing House opens the Old Book Fair on December 15.
 Life & Style
Life & Style
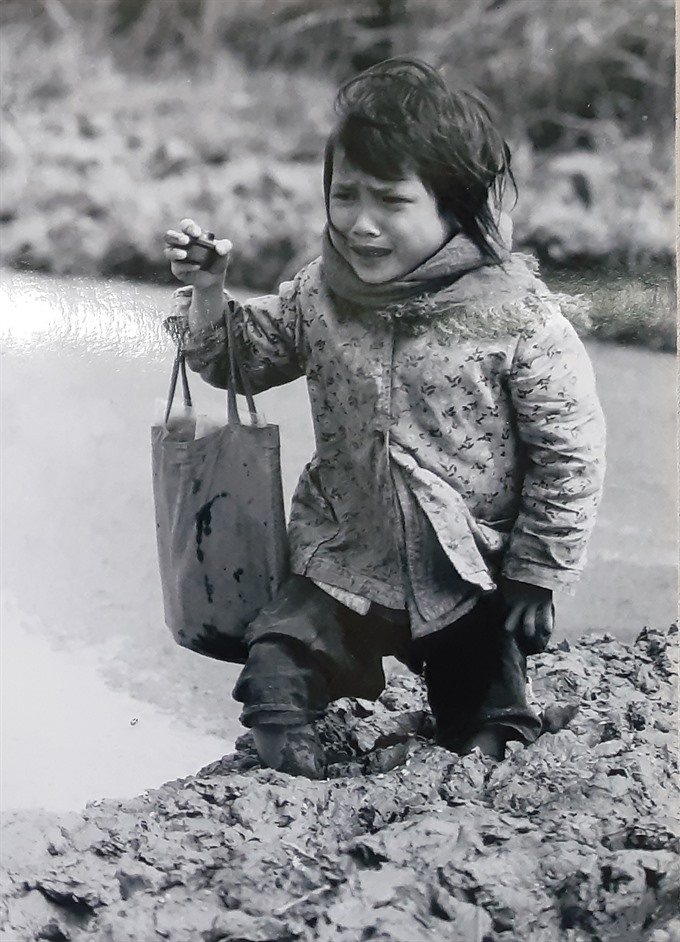
Hauting moments of the wartime, peaceful landscape of Hà Nội in the past and portraits of famous people who passed away are depicted in the photos displayed at an exhibition opened in Hà Nội yesterday.
 Life & Style
Life & Style
South Korean A-list actor Ahn Sung-ki will attend the South Korea - Việt Nam Film Festival’s opening ceremony on December 15 in Hà Nội.
 Life & Style
Life & Style
A duet concert by pianists Lise de la Salle and Thomas Enhco will take place at L’Espace in Hà Nội on Saturday.
 Life & Style
Life & Style
Berlin inaugurated a new addition to its UNESCO-listed Museum Island on Thursday, after a construction delay lasting several years and at costs that were twice the budgeted sum.






